Determining Your Personal Fat Threshold
Given the relevance of the Personal Fat Threshold to one’s metabolic health, it certainly would be nice if there was a way of knowing what your own threshold is. Unfortunately, there is no way to predict what one’s threshold is. There simply is no available tool that can reveal that information with any certainty.
Instead, there are only indirect methods of determining one’s Personal Fat Threshold. There are a few clues to determining what that point is for you.
Energy Distribution
First, some further background to understand why these markers are relevant. Recall that the Personal Fat Threshold is a theory that explains how much body fat one can store while still maintaining good health.
When your fat cells have become overstuffed, you develop insulin resistance. In that situation, further consumed energy (dietary carbohydrate or fat) has nowhere [safe] to go. This situation forces the body to further increase insulin in order to stuff the excess energy (in the form of fat) into your cells. When fat cells exceed their capacity, they die and break open, releasing a chemical signal that triggers inflammation.
In individuals with a high Personal Fat Threshold, the fat cells are able to divide (increase in number) rather than overfill. In contrast, individuals with low Personal Fat Thresholds are not able to expand their fat mass significantly, instead being prone to overfilling their existing fat cells.
Where does the excess energy go?
When the subcutaneous fat stores have reached capacity, excess energy spills over into the body’s circulation. The body will mount an insulin response to remove it from the bloodstream, forcing it to settle in whatever tissue is least resistant to insulin. Excess energy tends to contribute to visceral fat and ectopic fat, causing vascular disease, heart disease, fatty liver, etc.
Subcutaneous fat -> visceral fat -> ectopic fat
Clues to Personal Fat Threshold
Presence of Metabolic Disease
The simplest measure of whether you have exceeded your Personal Fat Threshold is whether or not you have evidence of metabolic disease, such as diabetes, pre-diabetes, cardiovascular disease (heart disease, stroke, etc.), fatty liver, etc. These conditions reflect the fact that your peripheral fat stores could no longer buffer you against the excess energy in your body; they could no longer partition off the energy surplus.
V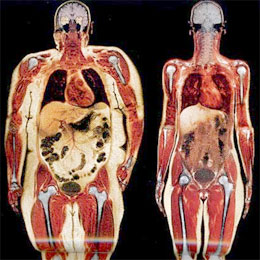 isceral Obesity
isceral Obesity
A key difference between individuals who are metabolically healthy obese (MHO) and those who are metabolically obese with normal weight (MONW) is the presence of visceral obesity. The presence of visceral obesity (excess intra-abdominal fat tissue) indicates that your body’s ability to expand your subcutaneous (peripheral) fat stores has been exceeded.
There are several methods of assessing visceral obesity, the best of which is direct imaging with either CT or MRI.
Genetic Predecessors
Given the genetic influence on the Personal Fat Threshold, it can be useful to look at the source of your genetics – your biological parents. What was their body fat content? Did they have metabolic disease?
While not an objective indicator, the metabolic health of your biological parents can give you a rough idea of what to expect for yourself.
It gets quite complicated, though, when considering the potential influence of epigenetics. Even beyond just what genes are passed on generation to generation, it turns out that certain genes can be turned on or off depending on environmental factors, i.e. one’s metabolic health. The on/off nature of these genes can also be passed along to one’s offspring.
Laboratory Data
There are several lab tests that help indicate when one is approaching or has exceeded one’s Personal Fat Threshold.
- Elevated fasting glucose
- Elevated Hemoglobin A1c
- Elevated fasting insulin
- Elevated triglycerides
- Low HDL
- Elevated TG:HDL ratio
- Small dense LDL (from NMR or VAP lipoprofile)
- Elevated inflammatory markers (e.g. C-Reactive Protein)
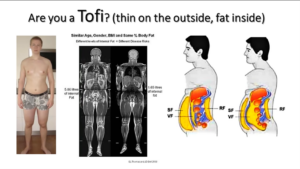
Skinny isn’t necessarily healthy
Given what we know about individualized capacity for fat storage, it’s important not to equate skinny with healthy. A major downside of doing so is the potential for delaying recognition of metabolic disease in someone who doesn’t fit the image of what we assume to be unhealthy. If we maintain an index of suspicion of metabolic disease only in individuals with obesity, we will inevitably miss a significant portion of affected individuals who fit the Metabolically Obese Normal Weight (MONW) phenotype, also commonly referred to as Thin-on-Outside-Fat-on-the-Inside (TOFI).
Regardless of body fat mass, an individual with metabolic disease must prioritize fat loss in order to move below the Personal Fat Threshold. Removal of the excess visceral fat and ectopic fat has a significantly favorable impact on overall metabolic health.
