Health Care has a Specialty Problem
Ever heard someone bemoaning the fact that they have multiple doctors? It’s the sad reality of the modern health care system, relying on multiple specialists to manage specialty-specific problems in parallel with other specialists. Oftentimes, a busy primary physician or non-physician provider will happily accept a role as gatekeeper and coordinator of this team of specialists. The health care systems strongly promote this model of care through incentivizing (or mandating) internal referrals, to the detriment of patient care.
The evolution of medical specialties
Once upon a time, among physicians there were only generalists. Now, there are more than 120 medical specialties. Specialist physicians were rare in the 1700’s, but became quite popular in the mid-1800’s, prompting a German physician visiting Paris to remark:
“Incredible! Each organ now has its own priest…and for some, they even have special clinics…”
Physicians started organizing themselves around organs, likely due to a desire and recognized need to expand medical knowledge. This trend towards specialization was, no doubt, important for the advancement of the science of medicine. I would argue, however, that we’ve let it go too far and are now suffering a problem of over-specialization.
Too many cooks in the kitchen
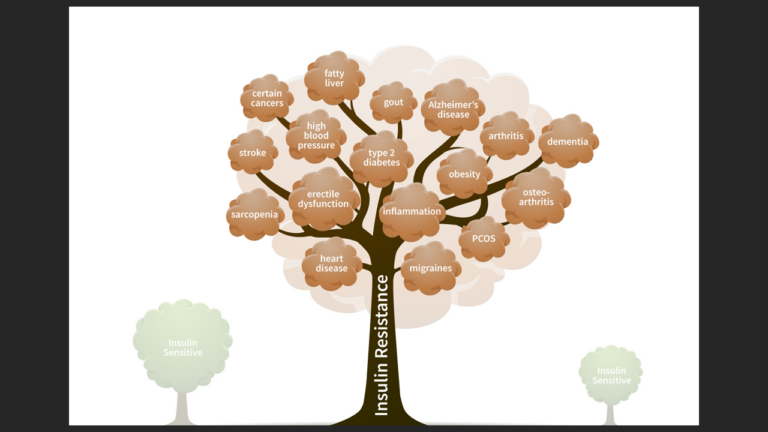
This problem of over-specialization is painfully evident in how modern medicine handles Insulin Resistance. There are a plethora of manifestations of Insulin Resistance, all of which have been assigned to different (often multiple) medical specialties. In some cases, there is a specialist who manages the primary manifestation (e.g. diabetes) and multiple other specialists who manage downstream complications (e.g. kidney disease, heart disease, neuropathy, eye disease, etc.).
For example, the most commonly recognized manifestations of Insulin Resistance are:
- Diabetes – endocrinology
- Obesity – obesity medicine, bariatric surgery, endocrinology
- Hypertension – primary care, cardiology, nephrology
- Cardiovascular disease – cardiology, cardiac surgery, vascular surgery, neurology, neurosurgery, interventional radiology
- Abnormal lipids – primary care, cardiology, neurology, lipidology
You get the point. There are many more manifestations of Insulin Resistance that the medical community does not openly acknowledge, like most cancers, dementia, inflammatory conditions, fatty liver, etc.
Impact of Insulin Resistance
It’s important to realize that the way these manifestations of Insulin Resistance are handled has an enormous impact on:
- The health care system – Insulin Resistance and associated conditions make up over 80% of health care
- The population – 93% of adults in the USA have poor cardiometabolic health
- The economy – in 2021, health care spending comprised 3% of the USA’s GDP.
- The world – USA guidelines have far-reaching impact
Harms of disjointed care
Assigning a different specialist to each manifestation of this disease process has resulted in disjointed care. Specialists tend to operate in a compartmentalized fashion, focusing only on their niche and wearing blinders such that they do not concern themselves with the big picture.

As an example, let’s say you suffer a heart attack and you receive care from a cardiologist. I trust that the cardiology team has done everything in its power to restore blood flow to your heart, but they soon declare their work done and turn you back over to your primary doc. Thus, you’ve addressed only one branch of a large diseased tree, and the remainder of the branches remain diseased – you still suffer from diabetes, obesity, sleep apnea, etc. Since the underlying disease is still running unchecked, chances are that you will be back in 5-10 years with another heart attack. Don’t act surprised.
Another problem with multiple cooks in the kitchen is that this approach has effectively resulted in multiple specialists all treating the same disease with different strategies. That’s frustrating to the other members of an individual’s care team; that’s beyond maddening to the patient who is getting all sorts of mixed messages and a cornucopia of pills to address each symptom. This situation markedly increases the chance of complications or medical error.
The way forward
Failing to recognize the common theme in modern health care has resulted in an inefficient, disjointed health care system. In order to make any meaningful long-term change, we must recognize and treat the underlying disease process, rather than parceling out treatment of each symptom.
That requires working with a forward-thinking physician who can see (and understand) the big picture. Avoid the short-sighted pill-prescribers who have a pharmacologic answer to every problem.
